The State of the Evidence in Religions, Health, and Development
Dr John Blevins
Emory University

Professor Esther Mombo
St Pauls University

This blog series is introducing and summarizing every chapter of the JLI’s 2022 Edition of the State of the Evidence in Religions and Development. The full report and chapters are available at their dedicated web page. A new blog on each chapter of the series will be regularly published during 2023. This is the second blog post in the series, focusing on religions, development, and health. The first blog that introduces religions and development evidence in general can be found here.
Work to improve people’s health is a significant part of development overall and religious institutions have both historically and currently played a significant role in healthcare. You may even hear stated that 70% of healthcare institutions in Africa are faith-based… except this is probably not true. This “evidence” on faith-based healthcare is unfortunately often misunderstood. It is a prime example of the ways in which we must be careful with evidence and not be satisfied with a quick statistic, as it may be misleading. There are many faith-based healthcare providers in Africa but the percentage varies from country to country. In fact, researchers have dug into the history of this 70% number and found “a process of ‘broken telephone’ whereby estimates are passed on and frequently distorted by policy- and advocacy-oriented influences at both the national and international levels.”
Given that the “evidence” can be misleading, what can we say about religions, health, and development therefore?
First, there are two key concepts to understand. “Religious health assets” are the assets “located in or held by a religious entity that can be leveraged for the purposes of development or public health.” Second, “beliefs and behaviors” are central to understanding religious influence on health. People of faith may experience contradictions between the teachings of their faith tradition, their own personal beliefs or actions, their worldviews about the phenomenon of health, and the health impact of their actions. It is because of religious health assets and the influence of people’s beliefs on their behaviors that it is necessary to pay attention to religions in health and development initiatives.
The historical influences of religion on global health and development practice have been significant. The earliest documented Muslim medical facilities were built in Baghdad in the 9th Century C.E. and over the next 500 years, Muslim hospitals were established across the Middle East, North Africa, Turkey, and Spain. In 1640, Roman Catholic missionaries established the first medical facility on the African continent. During the 19th century, Christian medical missionaries established facilities in British colonies across Africa, South and East Asia, Australia, and South America but by the start of the 20th century, American medical missionaries outnumbered their British counterparts and American Christian denominations were supporting over 1,000 health facilities. These efforts were carried out with an uncritical acceptance of Western cultural, religious, and intellectual superiority and medical missions provided a religious rationale not only for the development of global health and development institutions but also for colonialism.
By the latter decades of the last century, the secularization of public health and development fields had largely relegated religion to the margins. Some people started to raise the issue of religious influence in health and development again in the 90s and 00s. The creation of the International Religious Health Assets Programme (IRHAP), an international consortium of religious, health, and development practitioners and researchers, helped to coordinate a groundbreaking study with funding from the WHO in 2005 to map the contributions of religious health assets in Africa. Their work also focused on health systems strengthening, health services for those in extreme poverty, adolescent sexual health, and health and development policy. Researchers published a seminal special issue of The Lancet on Faith-Based Health-Care in 2015. The Lancet issue provided a benchmark on research in the field to date on topics such as faith-based health service delivery, the importance of partnerships across governmental, faith, and civil society sectors, and controversies in faith and health care.
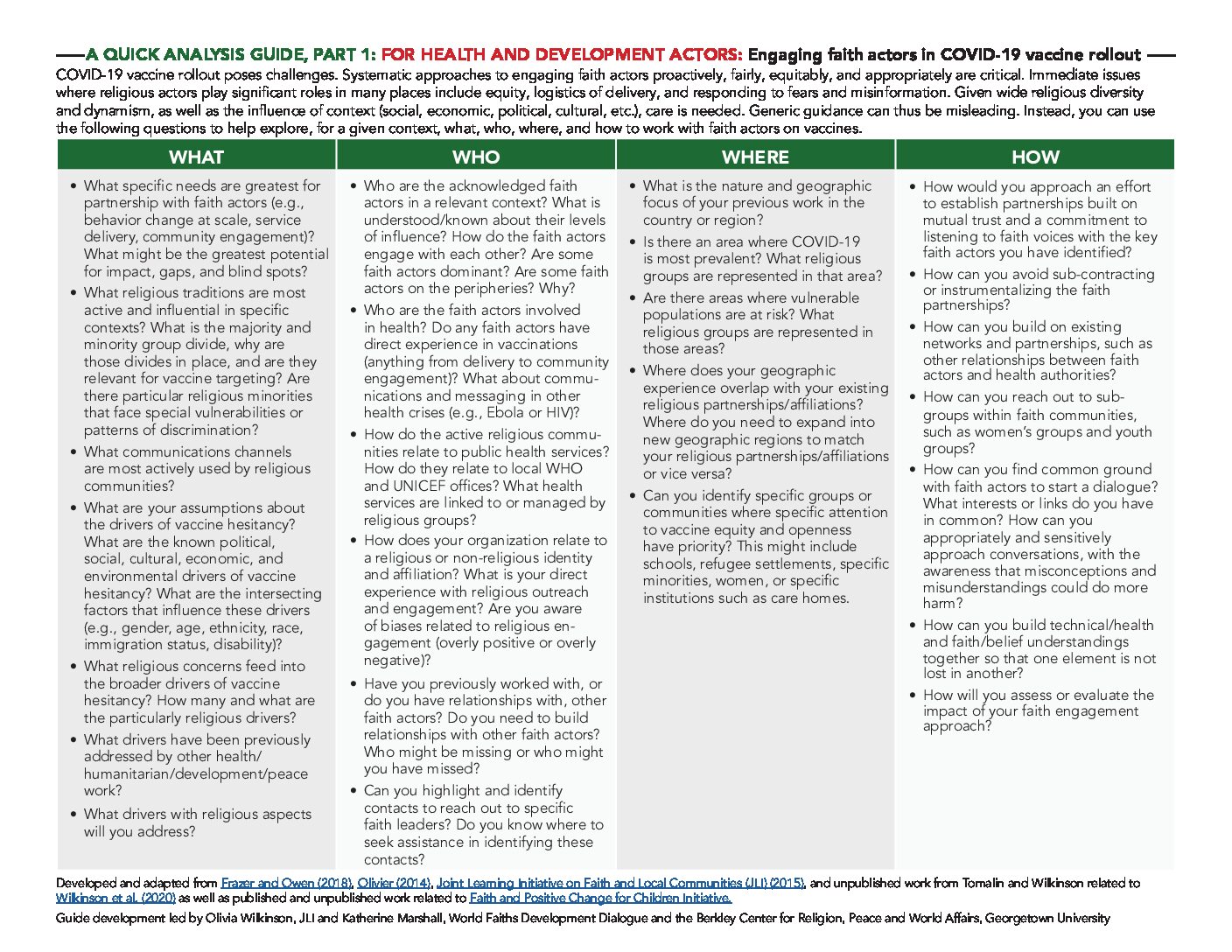
Sustained efforts to address HIV- related stigma and respond to pandemics have pushed researchers and policymakers to think more broadly about religion. Research into HIV/AIDS and religions has been a particular area of interest. The 2015 Ebola outbreak in Western Africa and the global COVID-19 pandemic have both demonstrated the distinctive ways in which religion can draw on deep reservoirs of trust. The initial public health Ebola response, calling for religious burial practices to be suspended without any input of religious leaders, was ineffective but when collaboration led to modified practices that allowed for safe burial while maintaining spiritual significance, infection rates dropped dramatically. Indeed, the trust and authority of religious leaders and through religious beliefs to influence health practices such as immunizations have been studied for decades. We have seen similar ways in which the authority of religious leaders has affected vaccine acceptance or hesitance during the COVID pandemic.
In the future, critical questions are unsettling some of the earlier work described above.
For example, Christian researchers and practitioners have examined “religious health assets.” Yet, we must ask: How do their own backgrounds bias what is seen or overlooked when considering what are tangible health assets? For example, white men from the US, Europe, and South Africa led much of this earlier research. How did their personal and collective experiences—experiences influenced by race, nationality, and gender—affect the ways in which they framed this research? How would women from East Asia, Central America, or East Africa describe those assets? These are some of the complex questions facing us as we seek to understand religion’s varied influences on health and development in the 21st century. 40 years ago, researchers, health and development practitioners and policy makers rarely considered religion in relation to health and development practice; a generation ago, the concept of “religious health assets” put religion back on the map. Today and for the foreseeable future, efforts to understand religion’s influences on health and development must not only focus on those assets but also address the complex questions about the power dynamics involved.

0 Comments